Quetiapine-Paliperidone LA
There are 2 switch possibities:
Number 1 (the general approach):
- Day 1: Switch to oral risperidone (or oral paliperidone): see this switch in the main cross table.
- Day 1-29: Maintain on oral risperidone (or oral paliperidone) and examine the effects.
- Day 30: stop oral risperidone (or oral paliperidone) and administer paliperidone-LA: see this switch in the main cross table.
Oral risperidone has better and more stable bioavailability properties than has oral 9-OH-risperidone=paliperidone. Food increases the absorption with 50-60% of the latter.
Number 2 (if a patient in the past reacted well on risperidon or paliperidone=9-OH-risperidone):
| ||||||||||||||||||||||||||||||||||||||||||
| ||||||||||||||||||||||||||||||||||||||||||
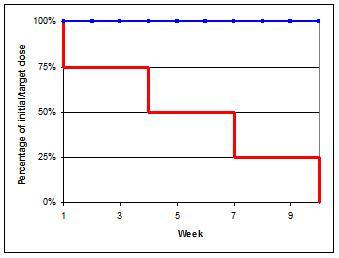
Switch medication from Quetiapine to Paliperidone_LA[5][6]
- Week 1-3: approx. 75% of initial dose
- Week 4-6: approx. 50% of initial dose
- Week 7-9: approx. 25% of initial dose
- Week 10: stop
- Day 1: Start depot according general dosing advice (Dotted line in graph)
- During this switch you could monitor ECG, especially in patients prone to QT-conduction problems.
- There is a possibility of QT interval prolongation.[7]
- Alternatively, first switch to oral form and then switch to depot to manage possible (adverse) reactions. With a direct switch to a depot it is advisable to administer a low testdose in order to exclude adverse reactions.

- ↑ 1.0 1.1 1.2 KNMP; Informatorium Medicamentorum 2023; Monografie "quetiapine" (Dutch)
- ↑ NVZA; Toxicology.org; Monografie 73 (dutch)
- ↑ Woods SW Chlorpromazine equivalent doses for the newer atypical antipsychotics J Clin Psychiatry 2003;64:663-667
- ↑ Drugs.com quetiapine-fumarate
- ↑ Switches are based on literature references on this page and expert opinions of the authors. The authors have used pharmacokinetic and receptor affinity properties to determine the switch schedules
- ↑ Stahl, S. M. (2013). Stahl's essential psychopharmacology: Neuroscientific basis and practical applications (4th ed.). Cambridge University Press.
- ↑ Stöllberger C, Huber JO, Finsterer J, Antipsychotic drugs and QT prolongation. Int Clin Psychopharmacol. 2005 Sep;20(5):243-51.
The editors of psychiatrienet.nl take the greatest care to provide up-to-date and accurate information on this site. Nevertheless, mistakes and omissions cannot be entirely excluded. No rights devolve from the information provided. The editors and other providers of information to this site accept no responsibility for the content of this site or for the information provided therein; neither do they accept responsibility for possible damages which may derive from the use of the information on this site or from the linked sites. The editorial board accepts no responsibility for the content of the (linked) sites, for access to them, or for the products and services on these sites, nor for the occurrence of errors, viruses, and/or disruptions in service.