Partial agonist-Paliperidone LA
There are 2 switch possibities:
Number 1 (the general approach):
- Day 1: Switch to oral risperidone (or oral paliperidone): see this switch in the main cross table.
- Day 1-29: Maintain on oral risperidone (or oral paliperidone) and examine the effects.
- Day 30: stop oral risperidone (or oral paliperidone) and administer paliperidone-LA: see this switch in the main cross table.
Oral risperidone has better and more stable bioavailability properties than has oral 9-OH-risperidone=paliperidone. Food increases the absorption with 50-60% of the latter.
Number 2 (if a patient in the past reacted well on risperidon or paliperidone=9-OH-risperidone):
| ||||||||||||||||||||||
| ||||||||||||||||||||||
Switch medication from Partial agonist to Paliperidone_LA[1][2]
Partial agonist is a collection of antipsychotic drugs having similar properties with respect to switching. A switch to member of the 'partial agonist' group from anotherdrug should be read as partial agonist-anotherdrug. Similarly, a switch from a member of the 'partial agonist' group to anotherdrug should be read as anotherdrug-partial agonist.
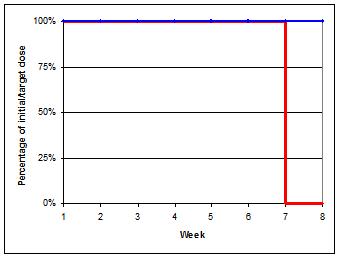
- Week 1-6: Continue drug at usual dose
- Week 7: Stop drug
- Day 1: Start depot according general dosing advice (Dotted line in graph)
- During this switch you could monitor ECG, especially in patients prone to QT-conduction problems.
- There is a possibility of QT interval prolongation.[3]
- Alternatively, first switch to oral form and then switch to depot to manage possible (adverse) reactions. With a direct switch to a depot it is advisable to administer a low testdose in order to exclude adverse reactions.

- ↑ Switches are based on literature references on this page and expert opinions of the authors. The authors have used pharmacokinetic and receptor affinity properties to determine the switch schedules
- ↑ Stahl, S. M. (2013). Stahl's essential psychopharmacology: Neuroscientific basis and practical applications (4th ed.). Cambridge University Press.
- ↑ Stöllberger C, Huber JO, Finsterer J, Antipsychotic drugs and QT prolongation. Int Clin Psychopharmacol. 2005 Sep;20(5):243-51.